







Arrival
Item
Download
Download
Item
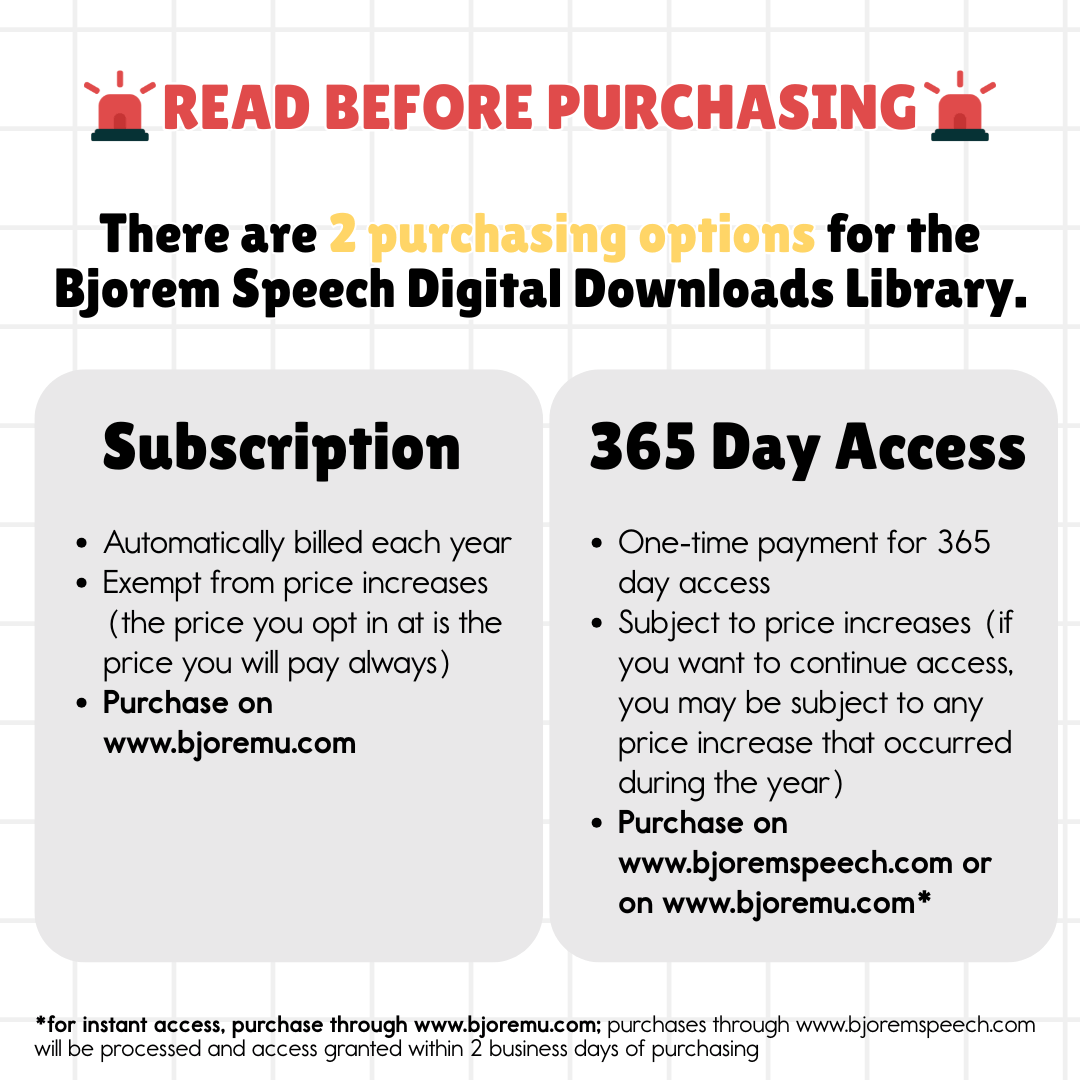
Option

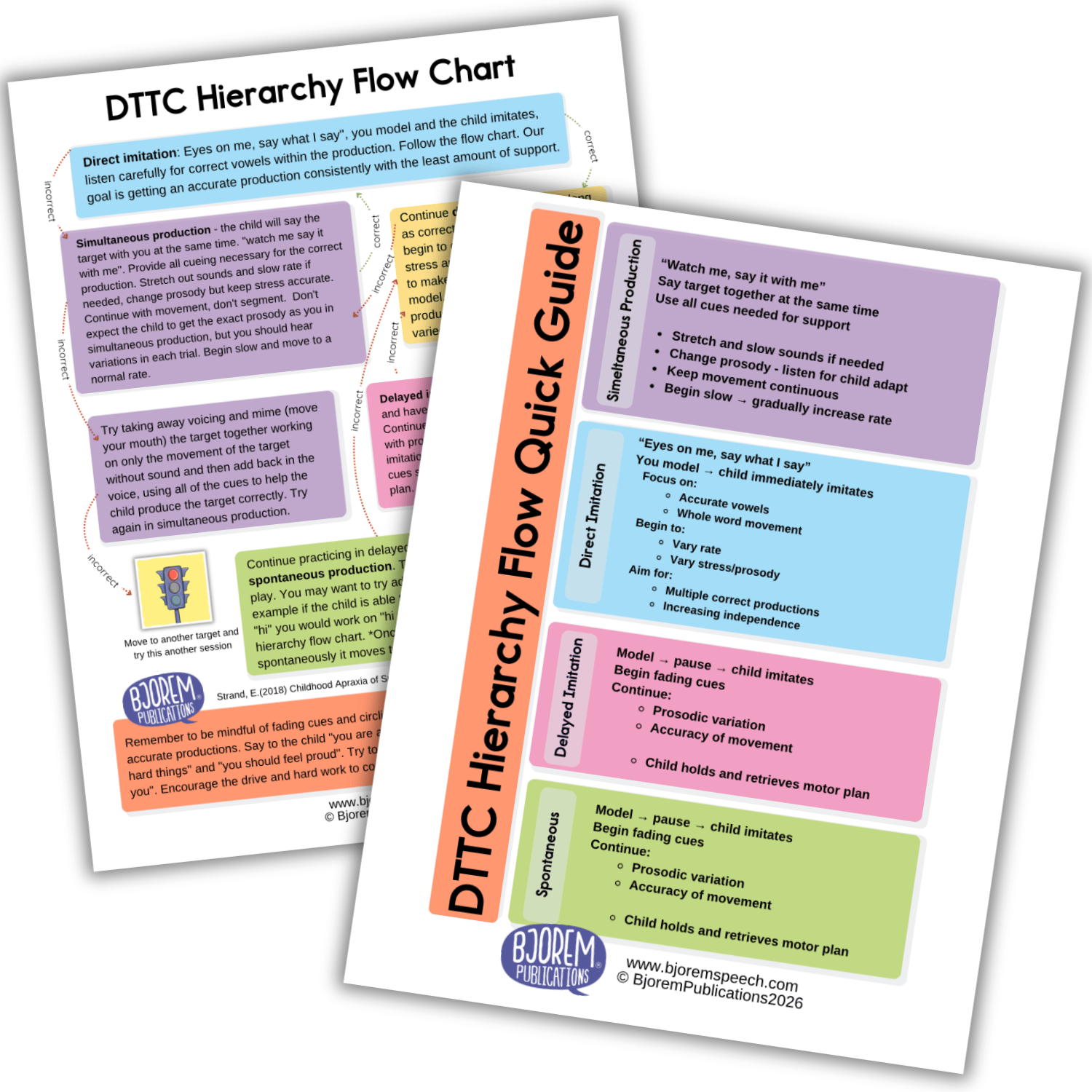
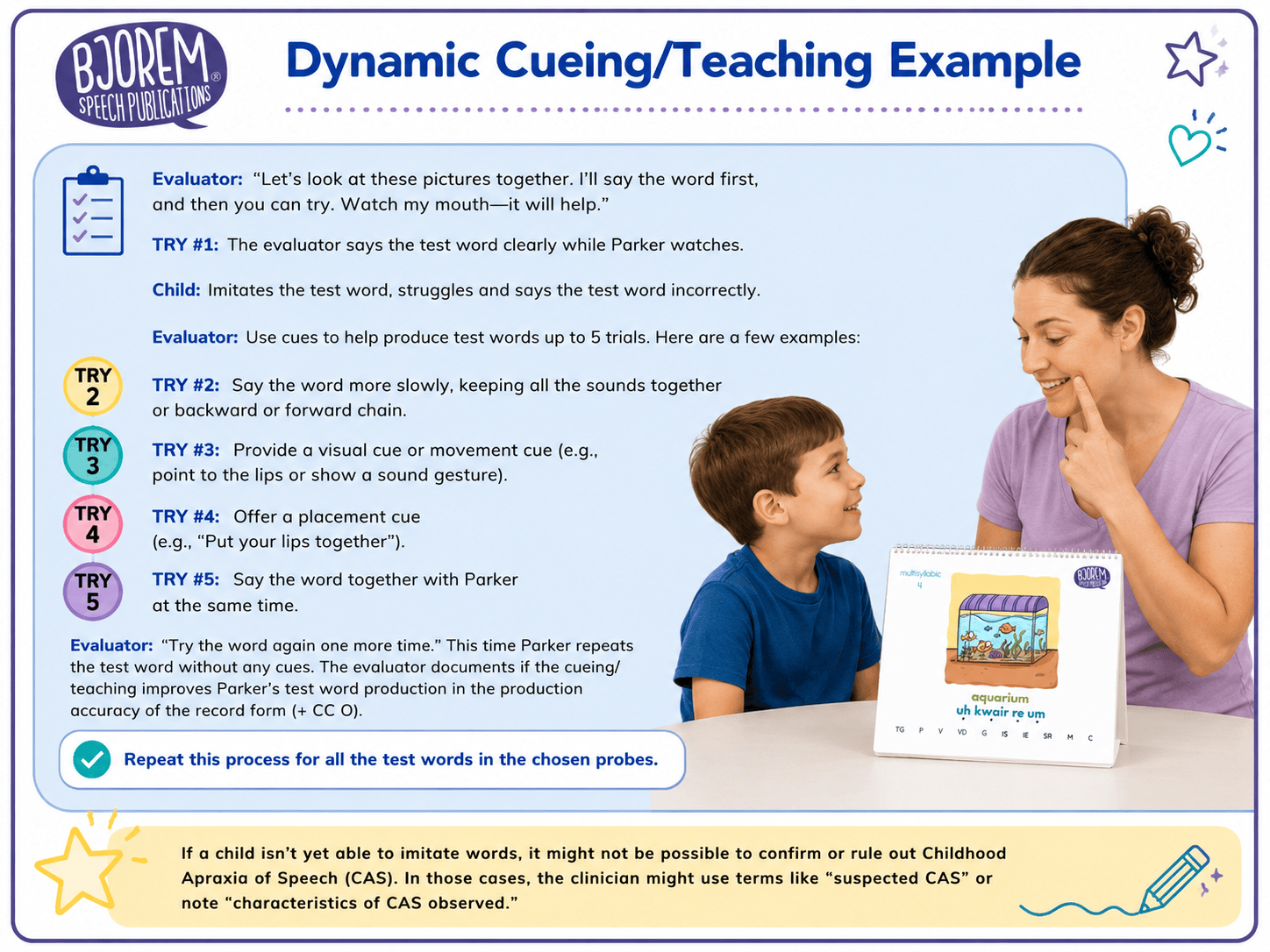
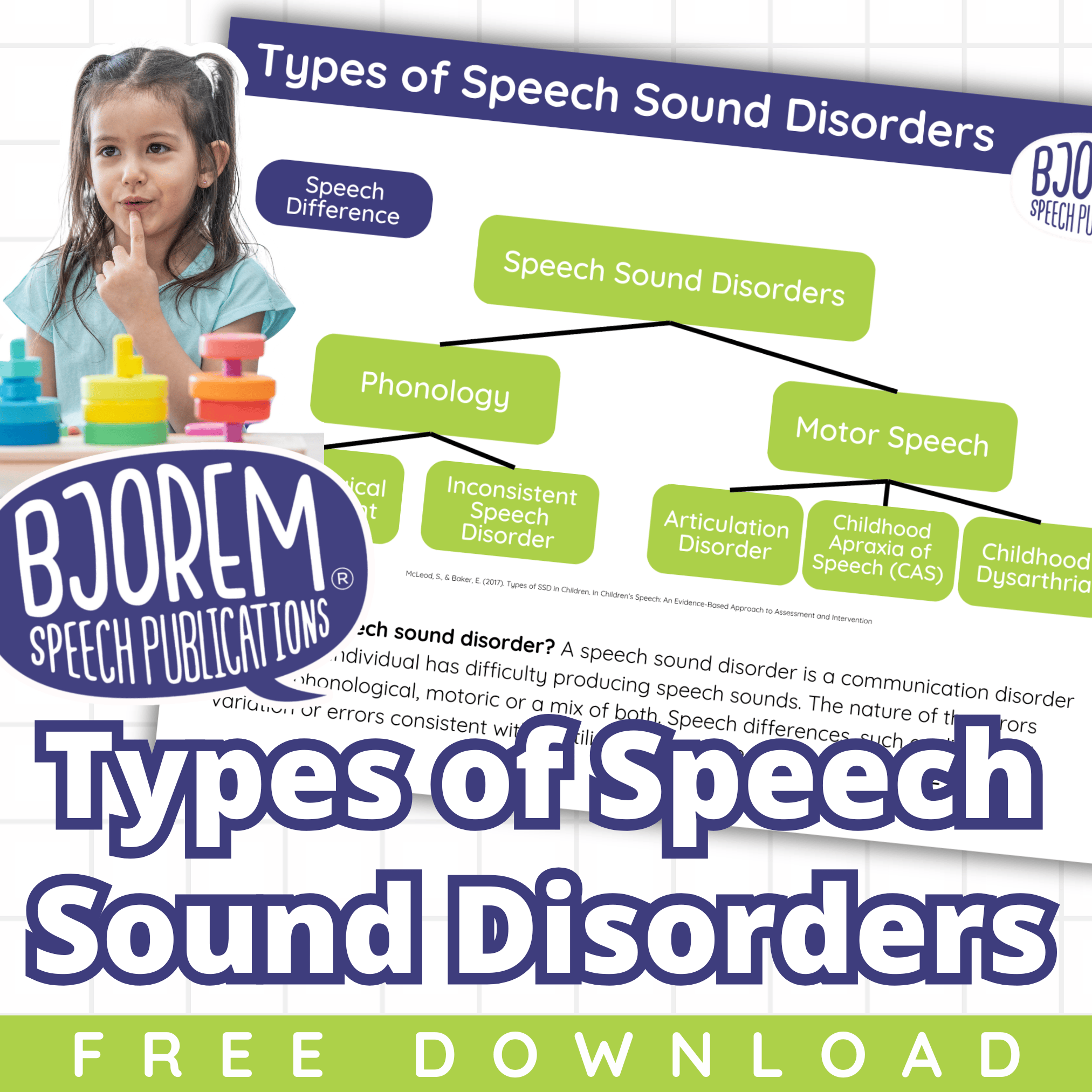
Childhood Apraxia of Speech
Explore Resources
Select a category below to begin:
Products & Tools
Expertly designed therapy products
Digital Downloads
Created for therapists
Courses
Take a course and earn PDH credits
Expert Advice
In-depth, professional articles
Events & Programs
Attend professional development events
Speaking Topics
Book an expert speaker
Videos
Watch videos on how to use our products
Research
The hows, whys, and backing
Childhood Apraxia of Speech
Products & Tools











Arrival
Item






































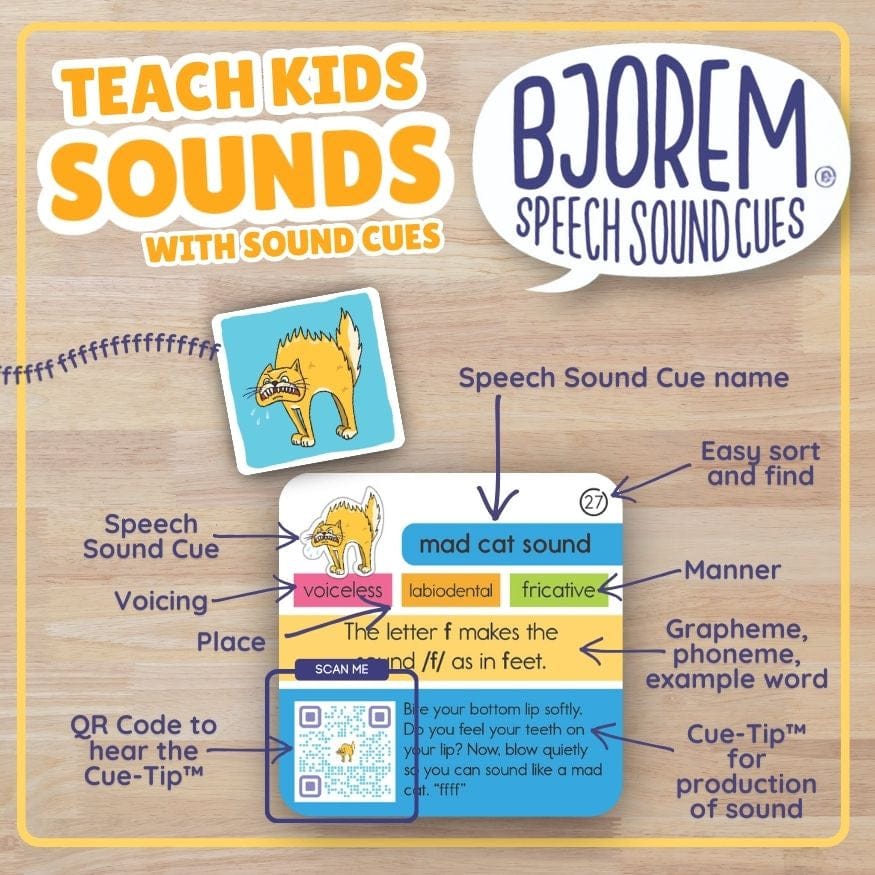
Bjorem PlayProof™ Poster: Bjorem Speech Sound Cues
Item
Arrival























































Digital Downloads
Download
Download
Download
Item
Download
Download
Item
Option
Download

Bjorem Publications Digital Gift Card
Download
Item


Download


Download
Download
Item
Option


Access
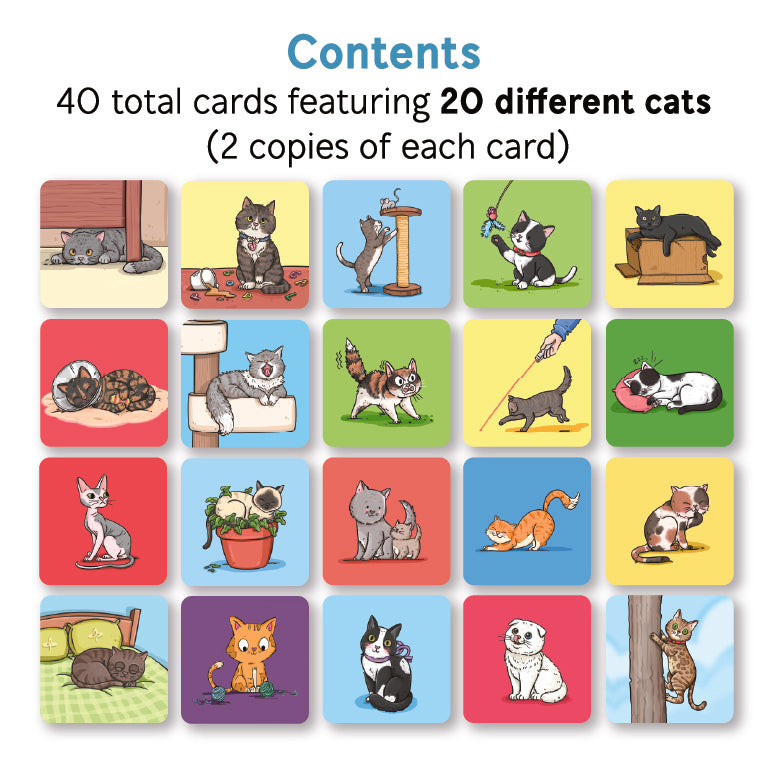
Bjorem® Stack of Cats: Cats Themed Picture Vocabulary Cards
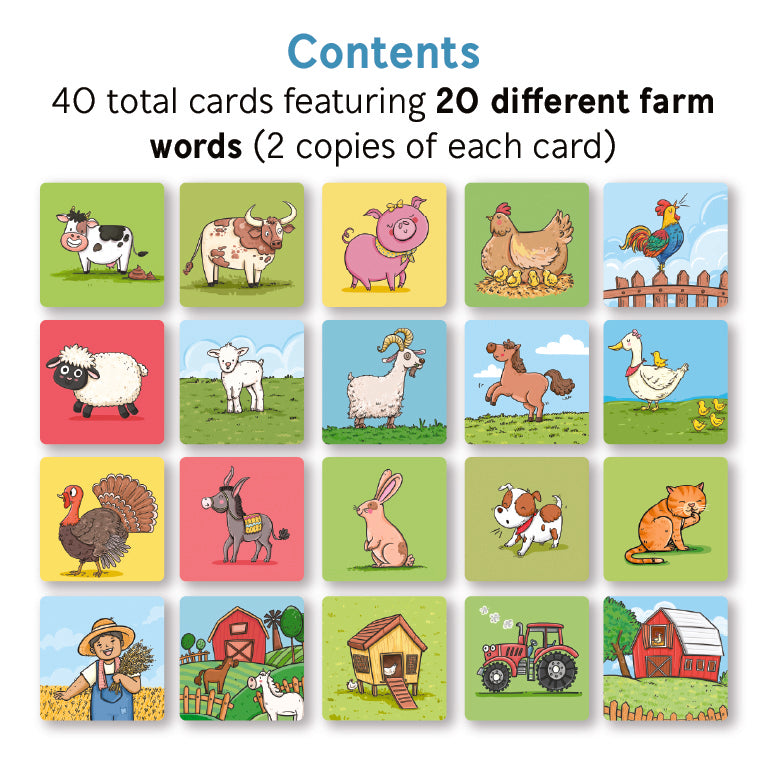
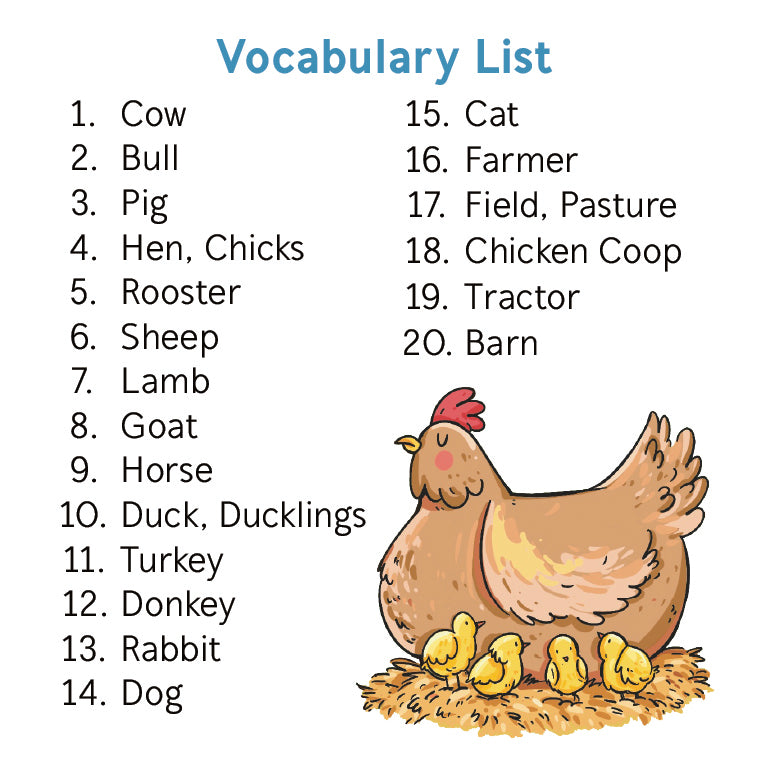
DING AND DENT: Bjorem® Stack of Farm: Farm Themed Picture Vocabulary Cards
Arrival
Childhood Apraxia of Speech
Courses & Webinars
Childhood Apraxia of Speech
Expert Advice

Childhood Apraxia of Speech
Events & Programs
Childhood Apraxia of Speech
Speaking Topics
Book a Bjorem public speaker to deliver a keynote at your event
6 Hours
Childhood Apraxia of Speech: Assessment, Diagnosis & Treatment
Led by Jennie Bjorem
In-Person Only
3 Hours
Assessment & Diagnosis of Childhood Apraxia of Speech
Led by Jennie Bjorem
In-Person or Virtual
3 Hours
Childhood Apraxia of Speech Therapy: Play-Based DTTC Focused
Led by Jennie Bjorem
In-Person or Virtual
1 Hour
Target Selection Using the VITAL Method Childhood Apraxia of Speech: DTTC Approach
Led by Jennie Bjorem
In-Person or Virtual
1 Hour
Characteristic Identification for Childhood Apraxia of Speech
Led by Jennie Bjorem
In-Person or Virtual
Childhood Apraxia of Speech
Watch Videos

What It Is

Identifying Issues

